


Wegovy for Cardiovascular Risk Reduction - Part 2

This is the Weight and Healthcare newsletter! If you like what you are reading, please consider subscribing and/or sharing!
In part one we looked at the staggering conflicts of interest and issues with the efficacy in the Semaglutide 2.4 (Wegovy) cardiovascular trial (Semaglutide and Cardiovascular Outcomes in Ob*sity* without Diabetes DOI: 10.1056/NEJMoa2307563) especially as compared to the deeply misleading claims in Novo Nordisk’s “company announcement” publicity stunt prior to publication.
Today we’re going to dig deeper into the data, what there is of it, anyway. As you are reading through this if you are tempted (as I would be as a reader) to ask “why don’t you just ask them for the data,” I want to share with you their data-sharing statement:
![Data Sharing Statement Lincoff AM, Brown-Frandsen K, Colhoun HM, et al. Semaglutide and Cardiovascular Outcomes in Obesity without Diabetes. N Engl J Med. DOI: 10.1056/NEJMoa2307563. Question Authors' Response Will the data collected for your study be made available to others? No Would you like to offer context for your decision? [X] The rest of the questions in the table are about how and when the data would be made available, but the authors have indicated that the data will not be shared.](https://substackcdn.com/image/fetch/f_auto,q_auto:good,fl_progressive:steep/https%3A%2F%2Fsubstack-post-media.s3.amazonaws.com%2Fpublic%2Fimages%2Fedb36a92-02a9-4213-8b17-bda8579eea4f_672x725.png "Data Sharing Statement Lincoff AM, Brown-Frandsen K, Colhoun HM, et al. Semaglutide and Cardiovascular Outcomes in Obesity without Diabetes. N Engl J Med. DOI: 10.1056/NEJMoa2307563. Question Authors' Response Will the data collected for your study be made available to others? No Would you like to offer context for your decision? [X] The rest of the questions in the table are about how and when the data would be made available, but the authors have indicated that the data will not be shared.")
I would characterize this trial as the most manipulative and opaque they’ve been with study data (and that, friends, is saying something.)
Note that in this piece I will refer to the Original Article (OA) and the Supplementary Appendix (SA).
I want to start with some of the claims they make:
”Overw*ight and ob*sity are independently associated with an increased risk of cardiovascular events, even after the influence of metabolic cardiovascular risk factors linked to excess weight has been accounted for.”
They are glossing over the fact that they did not account for the experience of weight stigma and weight cycling, both of which are more likely among higher-weight people and are also independently correlated with increased risk of cardiovascular events.
In part one, we talked about the misleading claim of a 20% reduction in Major Adverse Cardiac Events that appeared in a Novo “company announcement.” Now let’s look at the second two parts of their claim: that the risk reduction (which, spoiler alert, is actually 1.5% not 20%) was in “Adults with “overw*ight and ob*sity””
As I wrote in the previous piece, their trial criteria only included people aged 45 and older, with existing cardiovascular disease and without type 2 diabetes with a BMI of 27 or higher (while BMI is worse-than-useless measurement with a racist basis, since they are using it, I want to point out that the actual definition of “overw*ight” starts at a BMI over 25 not 27.)
Still, the study itself shows their use of “adults” to be even more misleading than it originally appeared.
OA Table 1 gives age data as a mean age of 61.6 +/- 8.9 (where 8.9 is the standard deviation.) From this, we can infer that two-thirds of subjects were between 54 and 71. SA Table S1 repeats the info above, and then gives a breakdown with percentages of subjects in age ranges (<55, 55-<65,65-<75, and ≥ 75) from this we can tell that 76.7% were older than 55.
What they don’t ever do is simply give the actual ages of the participants. I imagine that has something to do with trying to pass off a sample who were mostly over 55 and had an average age of 61.6 as “adults” but that’s purely speculation on my part.
72.3% of the subjects were [cis] men (there was no trans or nonbinary representation) and 83.9% in the semaglutide group and 84.1% in the placebo group were white.
This is an unconscionable lack of diversity and representation. Per the SA “The study was executed on six continents and in 41 countries” yet they still ended up 72.3% cis men and 83.9% white people in the treatment group??
Interestingly, in their 2-year (aka “long-term”) weight loss study, 77.6% were [cis] women (with, again, a failure to include transgender and nonbinary people) and also vastly overrepresented white people at 93.1%.
At this point I’ll just remind you (as we talked about in Part 1) that Novo Nordisk and the “academic steering committee” (with physicians who took over $7 million combined in payments from Novo Nordisk) designed the study so the question is whether or not they are poring over previous data they gathered on Semaglutide in other trials and trying to get a sample who would have the largest effect (for example, that cis white women would show the most, at least temporary, weight loss and cis white men would show the greatest cardiovascular reduction,) because it doesn’t seem that these seriously gender-skewed samples can be explained by differences of incidence of being higher-weight and or existing CVD in cis-men and cis-women, nor does it seem like anyone would (let alone should!) go to the trouble of running a trial on every continent but Antarctica and still end up with almost 85% white people.
But the group is even narrower than that.
Deb Burgard has pointed out “In SA Figure S5, the hazard ratios are not significant for women, Black people, Hispanic people, people over 75, and - big one - fatter people. OB*SITY PARADOX ALERT.” (Someday I’ll write a full piece on the “ob*sity paradox” but the super-quick explanation is that it’s a “paradox” that occurs when the assumption is that higher-weight people will have worse outcomes than lower-weight people, but they don’t.)
To qualify they had to have existing cardiovascular disease defined as “previous myocardial infarction, previous stroke, or symptomatic peripheral arterial disease“
In the actual study population, “more than three-quarters of the patients had had a previous myocardial infarction, and nearly one quarter had chronic heart failure”
So we’re back to mostly cis white men (it was also statistically significant for Asian men who were less than 10% of the study population) with a mean age of 61.6, on the lower end of the “overw*ight/ob*se” BMI scale., most of whom have already had a heart attack.
Or, as Novo Nordisk likes to call them “adults.”
Let’s dig a bit more into that 1.5% reduction in Major Adverse Cardiovascular Events.
OA Table 2 shows that while they were able to get statistical significance for their primary endpoint (which was a composite of death from cardiovascular causes, nonfatal myocardial infarction, or nonfatal stroke,) they did not achieve statistical significance for any of their confirmatory or supportive secondary endpoints, including the individual endpoints from the composite. (Their use of NA is misleading here because the p-values were available, they simply chose to take these endpoints in order and then not calculate statistical significance after the first non-statistically significant result which was the first one. A quick reminder statistical significance is NOT a measure of importance or size of effect, which is why the 1.5% reduction qualifies. It’s simply a statistical test of whether that 1.5% reduction is more likely due to the intervention or simply due to chance. For a refresher on statistical significance, head over here.)
Let’s look at the claim from the “company announcement” saying that “Semaglutide 2.4mg” was responsible for the effects of the trial (such as they are.)
SA Figure S1 shows that 6.1% of the treatment group didn't complete the trial due to adverse events, but 26.7% of the 8,803 people (2,361 subjects) in the treatment group didn't complete the treatment which meant they were included in the trial but did not manage to stay on the drug (and the study authors gave themselves a 29-day efficacy cushion since “treatment discontinuations that occurred less than 30 days before the end-of-treatment visits were not counted.” )Again, about twice as many people didn’t complete treatment due to adverse events in the semaglutide group than the placebo group.
SA Figure S2 shows that while they started off with 8,803 in the Semaglutide and 8,801 in the Placebo group, they ended at 48 months with only 712 in the Semaglutide group and 708 in the Placebo group at which point the graph just…stops. (They explain below that they’ve truncated the graph “due to the limited number of patients after 48 months.”) This means that while they repeatedly refer to an “end-of-treatment visit,” and the trial was scheduled for 59 months, they’ve chosen to simply not show us the data from 48 to 59 months. This attrition seems especially significant to me, given the fact that the medication is meant to be taken for the rest of a patient’s life, but they had lost so many people 4 years in that they threw in the towel on sharing data.

The body weight numbers in SA figure S6 are even worse, showing that at 2 years they’d lost 39% of participants and at 4 years they’d lost about 90% of participants, though they went ahead and graphed the weight loss over time like it was a meaningful number, not asking if the people who stopped doing the weigh-ins were people who were not losing/losing less weight.
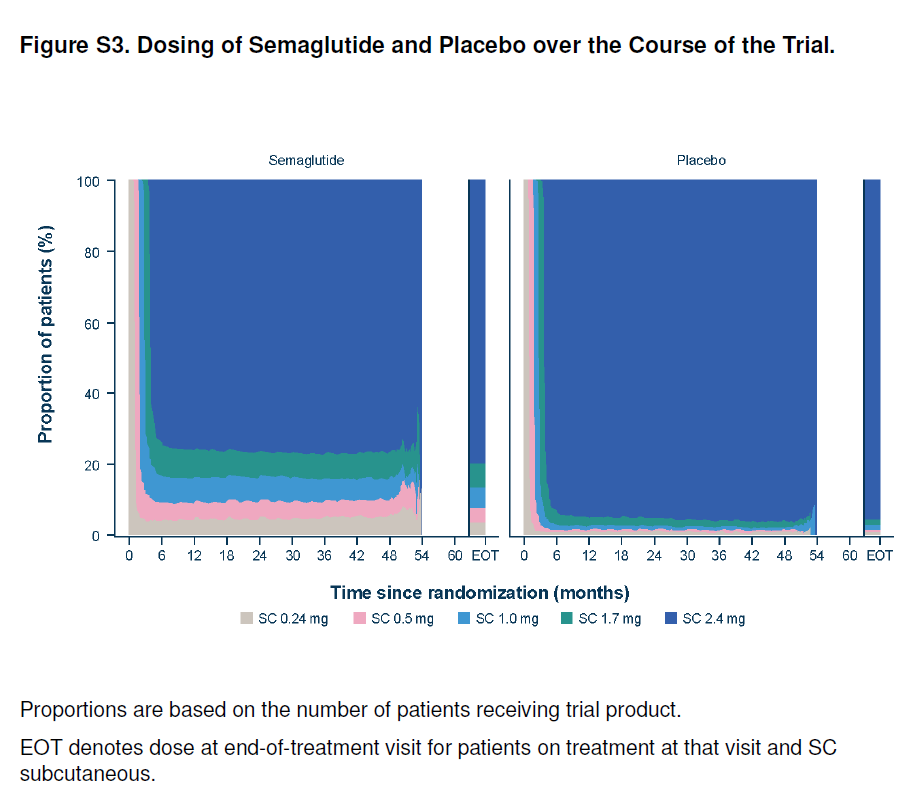
In terms of dosing and titration, the study included (as all Semaglutide use does,) a dose escalation schedule. It started with a .24mg non-therapeutic dose (this is a dose that is not expected to have a medical impact other than to help the body get used to the drug prior to dose escalation.) I feel like I should mention that this is… odd, since the standard initial dose is .25mg in every other study and prescribing instruction (it’s a pre-filled pen.) I thought it was a typo initially but it is stated repeatedly so I don’t know what that’s about. At any rate, per the OA:
“The starting dose of semaglutide was 0.24 mg once weekly, and the dose was increased every 4 weeks (to once weekly doses of 0.5, 1.0, 1.7, and 2.4 mg) until the target dose of 2.4 mg was reached after 16 weeks. If dose escalation led to unacceptable adverse effects, the dose-escalation intervals could be extended, treatment could be paused, or maintenance doses below the 2.4 mg per week target dose could be used”
According to SA Figure 3, around 25% of people in the treatment weren’t on the full dose the majority of the time, dose de-escalations spiked between 48 and 54 weeks, and around 5% never even made it off the non-therapeutic .24mg dose (and I say “around” because instead of actual numbers they gave us this weird graphic, divided up by 20’s on the y-axis.) This is more misleading since the number of patients was steadily going down over the time period shown here.
So Novo claimed in the company announcement that “Semaglutide 2.4 mg reduces the risk of major adverse cardiovascular events by 20% in adults with overw*ight or ob*sity in the SELECT trial.”
In truth, Semaglutide at various dosages reduced the risk of a composite of three major adverse cardiovascular events (but not individual ones) by 1.5% in white men with an average age of 61.6 years old at the lower end of the 27+ BMI range who had existing heart disease and did not have Type 2 Diabetes.
They got what they wanted. Wegovy to reduce cardiovascular risk was given Priority Review status and seven months after Novo’s alternative-fact-filled “company announcement” the FDA approved Wegovy (the weight loss dose of Semaglutide) for “Adults with overw*itght and ob*sity and existing heart disease.” This is a much, much bigger group of people than were actually shown to have even the 1.5% reduction in the composite of cardiovascular events.
Beyond the issues with what is there, I also want to mention what’s not there. First of all, they didn’t test or striate for the effect of lower doses of Semaglutide, even though it comes in doses much lower than 2.4mg. I wonder if that’s because 2.4mg is the weight loss dose (Brand name Wegovy) and they wanted to use this study (and subsequent FDA approval) as part of their huge campaign pushing for insurance coverage of Wegovy. Given the small effect and the number of people in the treatment group who didn’t make it to the 2.4mg dose, it’s entirely possible that a similar reduction could be created at lower doses with fewer side effects and, thus, fewer people discontinuing the drug. If so, even though it would still be a small effect in a narrow demographic, that means that it could help more people at a significantly lower cost.
The Semaglutide and Cardiovascular Outcomes in Patients with Type 2 Diabetes study, doi: 10.1056/NEJMoa1607141 further legitimizes this question. In this study participants with diabetes were given doses of .5mg or 1mg or a placebo and they had an absolute risk reduction of 2.3% (6.6% in the semaglutide group 8.9% in the placebo group) for the same composite outcome.
Also, there is no weight-neutral comparator group, meaning we have no way of knowing if weight-neutral, health-supporting interventions would have given the same or greater benefits with far fewer risks (as research suggests they may) and at significantly (and I don’t mean statistically significantly) lower cost.
This question is legitimized by part of the discussion in the OA of this study that says “a post hoc analysis of data from a previous trial has suggested that cardiovascular risk might be decreased among patients who lose at least 10% of their body weight…However, the data are consistent with the between-group difference in the incidence of cardiovascular disease emerging early in this trial, which suggests that more rapid treatment- induced physiological changes beyond the magnitude of body-weight loss may have mediated at least part of the cardiovascular benefit.” In other words, the impact happened before much of the weight was lost.
As always I take a firm view of bodily autonomy and I am not, in any way, trying to shame people who choose to take this medication. I do want people to have accurate information that isn’t bought and paid for by Novo Nordisk.
Just as a final thought, when I talk about issues with research like this – including to healthcare audiences – often the response I get is “that’s just how research is.” I want to say that’s a completely natural response, but I feel it’s also a part of the problem. I think that when we shrug off, or rush to justify these egregious research practices instead of holding all of those responsible (the pharma companies, the researchers, the FDA etc.) accountable, we end up aiding and abetting them. And whether it makes a difference or not, I choose to say something because I think it’s the right thing to do.
Did you find this post helpful? You can subscribe for free to get future posts delivered direct to your inbox, or choose a paid subscription to support the newsletter (and the work that goes into it!) and get special benefits! Click the Subscribe button below for details:
Liked the piece? Share the piece!
More research and resources:
https://haeshealthsheets.com/resources/
*Note on language: I use “fat” as a neutral descriptor as used by the fat activist community, I use “ob*se” and “overw*ight” to acknowledge that these are terms that were created to medicalize and pathologize fat bodies, with roots in racism and specifically anti-Blackness. Please read Sabrina Strings’ Fearing the Black Body – the Racial Origins of Fat Phobia and Da’Shaun Harrison’s Belly of the Beast: The Politics of Anti-Fatness as Anti-Blackness for more on this.
It's even worse than I thought. Thank you for taking so much care to explain all of this.
One of my favorite passages:
"So we’re back to mostly cis white men with a mean age of 61.6, on the lower end of the “overw*ight/ob*se” BMI scale., most of whom have already had a heart attack.
Or, as Novo Nordisk likes to call them “adults.”
Even though I'm feeling a bit rocky right now (going through antidepressant withdrawal in preparation for new adhd medication and feeling darn ambivalent about that), I am near tears, nay, tears are dripping down my face, at the ongoing saga of pharmaceuticals trying to make money off of normal human beings through statistical malfeasance and all the other shortcomings that become obvious once their work is under the spot light. Don't be surprised if you hear that I've been taken in by the white coats for walking naked through my neighborhood shouting, "I'm mad as hell and I'm not going to take it any more!" followed by "a reverence"* to you, Ragen. (*Once upon a time, before puberty, I was a cute thing in a pink wrap leotard and pointe shoes making such to a matronly teacher from the Joffrey Ballet.) I just dare my PCP to make any more suggestions about any kind of drug therapy for any symptom I have. IMAHAINGTTIAM!!!!!!!