


Weight Loss Surgery - Long-Term Outcomes and Informed Consent
Weight Loss Surgery Part 3

This is the Weight and Healthcare newsletter! If you like what you are reading, please consider subscribing and/or sharing!
In part one and part two of this series I alluded to the lack of information on long-term outcomes of these surgeries. The truth is that beyond ten years we have very little information about outcomes, which makes an informed consent conversation difficult, if not impossible. In the final part of this series we’ll look at long-term outcomes and informed consent, with the understanding that what I’ve provided in these three pieces is not even close to all there is to discuss, it’s just a foundation and I’ll no doubt write more about this moving forward. If you are looking for a more detailed discussion of the risks of the specific types of procedures, you’ll find that here.
As I mentioned in parts one and two, while I am solely responsible for the content here, my work around these surgeries has been deeply influenced and supported by the work of others including and especially Deb Burgard and Lisa Du Breuil.
Content note: There will be frank discussion of the harm inflicted by these surgeries, including self-harm. Also, a note that where studies are written from a perspective of, or containing, weight stigma I don’t link to them, but I do provide enough information for them to be found online if someone wants to search.
Before I dig into it too far, one surgery I haven’t discussed much in parts 1 and 2 is the Lap Band procedure, so I wanted to take a moment on it now. The reason I’ve not spent much time on it is that this surgery is falling out of fashion. In summary, these surgeries bind the stomach to make it smaller to force food restriction. They pose serious risks to patients and have a high rate of people regaining to, or close to, baseline. They also have high complication and re-operation rates (some studies show it as high as 60%.) A study by Ibrahim et al. looked at Medicare patients who got the procedure between 2006 and 2013. They found that by 2013, 77.3% of the money that Medicare was spending on gastric banding was for re-operations. They are often marketed as reversible but, in fact, the bands can be complicated and difficult to remove, and the removal can leave people with lifelong physical and psychological harm. Again, I don’t believe that these surgeries meet the requirements of ethical, evidence-based medicine, especially when compared to weight-neutral healthcare options.
Moving on…
In part two I included Dr. Paul Ernsberger and Sandy Swarzc’s list of side effects and, as long as that list is, they aren’t the only ones. In their paper “But Everything Is Supposed to Get Better After Bariatric Surgery!” (TW for discussion of self-harm and suicide) Lisa DuBreuil et al. examine the research around increased risk of suicide and self-harm post-surgery, as well as examining possible mechanisms, which include decreased quality of life post-surgery, post surgery weight gain, health conditions that are only temporarily improved by the surgeries and then recur, unrealistic expectations of the surgery, and self-blame for these (well known) possible negative outcomes. They also discuss how misleading marketing of these surgeries can be, including how selling them as a “cure-all” sets patients up for negative psychosocial impacts after the surgeries. For example, they point out that despite strong evidence of increased risks of alcohol abuse and suicide, the American Society for Metabolic and Bariatric Surgery listed these risks as “misconceptions” on their website.
In terms of research on long-term outcomes there is almost no research that even looks past ten years (and, as I mentioned earlier, I’ve been told by several medical grant writers that there is absolutely no interest from funders, including the NIH, in doing so.) Let’s look at some of the very few examples that exist:
In 2019, Anita Berg published “Untold stories of living with a bariatric body: long-term experiences of weight-loss surgery” which looks at the stories of seven people who had the surgery.
I first want to note that Berg’s piece is, in many ways, written from a position of uncritical weight stigma. First, Berg accepts at face value the pathologization of larger bodies. She also claims that bariatric surgery “is currently the most effective treatment for achieving permanent weight loss and improving comorbidities for severely ob*se patients” without noting (perhaps without knowing?) that the studies she cites do not compare the surgeries to weight-neutral health-supporting interventions, and don’t thoroughly examine long-term outcomes.
In the first couple of years post-surgery (what is often known as the “honeymoon period,”) patients reported positive experiences. However, predictably, the honeymoon period ended and negative experiences increased. For example, after eight years none of Berg’s subjects were able to reliably predict what would trigger dumping syndrome (also known as rapid gastric emptying,) a violent biological response to type and/or quantity of food consisting of vomiting and sometimes diarrhea which can cause irregular heartbeats.
One participant who had reached her “goal weight,” stated “Now, after surgery, I wonder…am I really better? I am 35 years old, having high risk of osteoporosis, blood pressure problems and all kind of things. Disorders I am used to in my job at the nursing home, at 70+, so what is happening?”
In a sentiment that echoes what I have heard time and again from survivors of these surgeries, one participant explained “I would not have done the operation again. I'd rather be locked up in a prison cell with locked jaws… because you're very plagued afterwards…”He revealed “I have had several suicide attempts. They did not know what gastric bypass was. What is it? What is it? Once they had to use Google. Then I thought, what the hell have I done?… I've been so far down that I've wanted to kill myself.”
Berg notes that not only are there negative health outcomes, but that because of the perception of having given “informed consent” patients tend to blame themselves for those negative outcomes.
I want to note, again, that the mobility and health improvements that patients saw short-term may well have been achievable (with dramatically less risk) through weight-neutral interventions.
These two studies (which are of the same cohort) are frequently used as examples of long-term outcomes:
Effects of Bariatric Surgery on Mortality in Swedish Obese Subjects
Lars Sjöström et al.
Life Expectancy after Bariatric Surgery in the Swedish Obese Subjects Study
Carlsson et al.
These studies compare a group of people who were given medical (non-surgical) “interventions” for “ob*sity”* to a group who had weight loss surgery. They have high follow-up rates on mortality because they were able to use records to find out when/if people died, even if they dropped out of voluntary study follow up. The issue, though, is that people (of all sizes) die for lots of reasons, but if you assume that all people who are fat died of…fatness, then you create biased research.
In terms of follow-up beyond just mortality, the dropout rate in the surgical group is significantly higher than in the control group (by about three times) so we are missing a significant amount of data about outcomes in the comparison. Moreover, we don’t know why these subjects dropped out and, given the risks to quality of life posed by these surgeries, it is disturbing to me that “what happened to these people?” is not a question the study authors seemed interested in even posing, let alone answering.
I also note that in their explanation of the medical (non-surgical) “treatment” they explain: “No attempt was made to standardize the conventional treatment, which ranged from sophisticated lifestyle intervention and behavior modification to no treatment whatsoever.” Given the issues with weight loss as a “treatment” (near complete failure rates, weight cycling, psychological harm, etc.) the deaths among the non-surgical group may be linked to their attempts at weight loss. I think it’s also significant that this study doesn’t have a group for weight neutral interventions, but given the research on the ability of weight neutral interventions to improve health, this study does not, to me, support the idea that surgery is a “better option” since the “control” group was pretty out of control, and there was no group with weight neutral health supporting interventions.
In the second study, the surgical group’s life expectancy is still 5.5 years less than general population. Since the control group’s life expectancy is subject to the dangers of weight loss interventions, which are associated with higher mortality, and since studies show that the risks for all-cause mortality and health hazard ratio can be attenuated or eliminated by weight-neutral interventions, I have to wonder where the life expectancy of a weight neutral group would fall.
Moreover, there is still the serious question of quality of life. We don’t know if those who lived a few years longer were part of the group of patients who survived the surgery but were miserable, plagued by horrific side effects, and desperately wishing they could take the surgery back.
Finally, Deb Burgard has pointed out that it’s important to look at the “number needed to treat” or NNT. That is, the number of people who need the get intervention (in this case, the surgery) in order for one person to experience the desired outcome. In this study the NNT to prevent one death over the next 20 years (vs what would happen with "regular medical management") is 35. So (taking the study info at face value) 35 people with a BMI greater than 39 would need to have the surgery (and take on all the risks) to prevent one death (though the person whose death would have been prevented would have an undetermined quality of life.) [Note - this section has been edited from the original to correct my misunderstanding of Deb’s initial quote.)
This number is alluded to in the main paper but the actual information is buried in the supplemental material. Here is a screen shot:
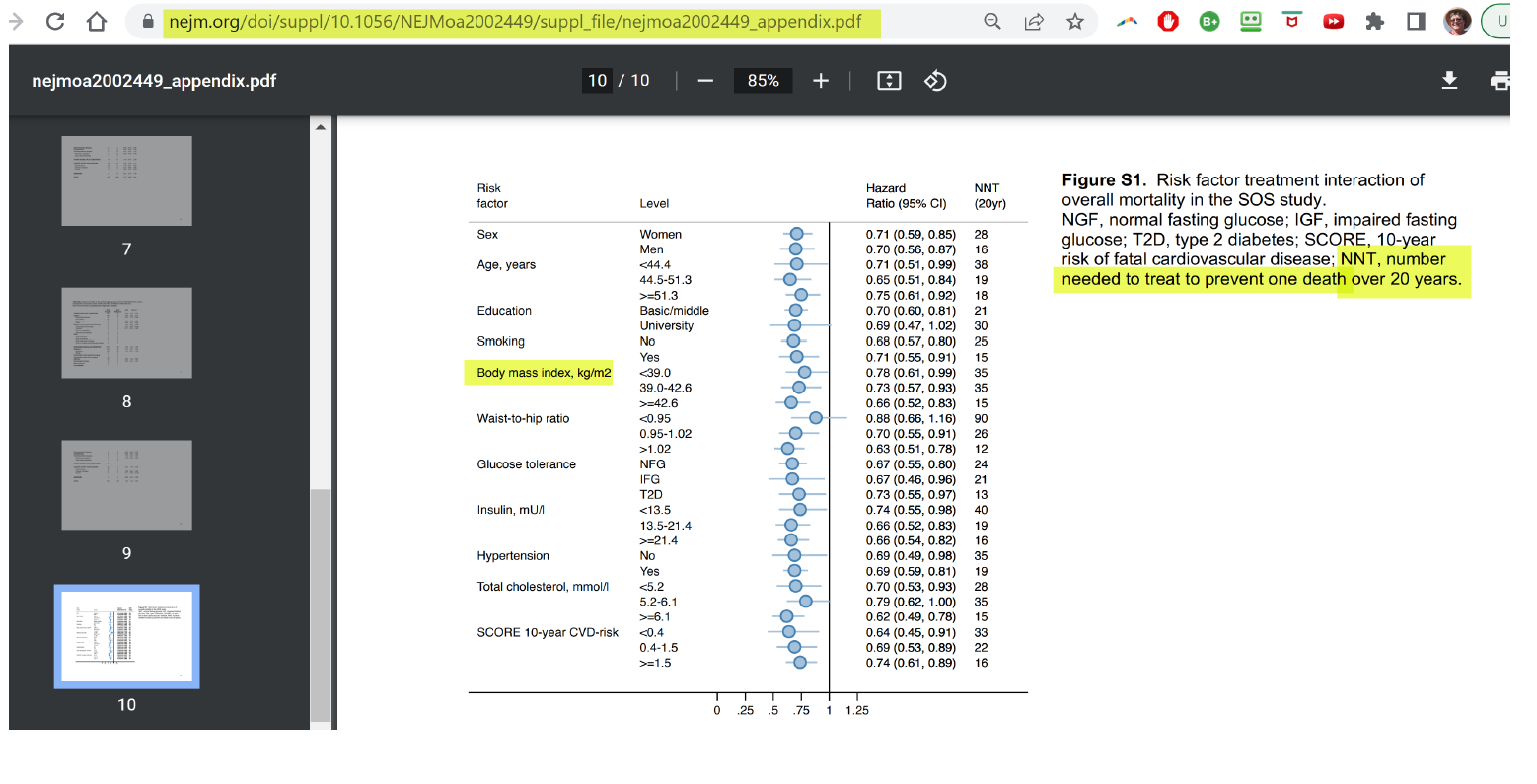
Again, given the risks of these surgeries, I don’t believe that this study supports them as an ethical, evidence-based intervention.
Informed Consent/Shared Decision Making for Weight Loss (Bariatric) Surgery
Given the combination of the aggressive marketing of these surgeries (including by practitioners, companies, and astroturf organizations with a profit interest) and the severe lack of knowledge about long-term outcomes for these patients, the concept of informed consent and shared decision making becomes extremely questionable.
I don’t believe that these surgeries meet the requirements of ethical, evidence-based medicine. That said, I am aware that some healthcare practitioners will continue to campaign for their use. Due to that, and as a harm reduction model, I offer the following.
First, at the very least, they should be considered only as an absolute last resort once all options for medical management (including and especially weight neutral medical management) have been exhausted.
Even then, they should require a serious and lengthy informed consent/shared decision-making process, undergone from the perspective that this is an informed consent process for a major surgery, not a marketing spiel. The discussion should include (based on the surgery offered):
Explaining that this procedure takes their currently healthy digestive system, and surgically puts it into a disease state
Explaining that the data shows that, while the surgeries may offer health benefits (including improved glycemic management) in the short to mid-term, there is a serious lack of data about long-term outcomes, meaning that when it comes to long-term outcomes, this is essentially an experimental procedure
Explaining that, in fact, their long-term health and quality of life could be worse (including far worse) after having the surgery than it would be without it
Explaining that short term health benefits may be lost, additional conditions may develop, and weight may be regained, that they may experience post-bariatric hypoglycemia that can be life-threatening, and that, no matter what, their digestive system will never return to its current, correctly functioning, state
Truly addressing the long-term financial costs of the surgery including supplementation, and being clear if the surgery means that they will no longer be able to meet their nutritional needs through food alone, and, if so, that if they stop taking the supplements (including if they are ever in a financial position in which they cannot afford them or don’t have access to them) it could have serious, possibly life-threatening consequences.
A frank discussion of body changes after surgery including the likelihood of loose skin (preferably with pictorial examples) and the fact that even if it is causing serious physical and/or psychological discomfort, the surgery(ies) to correct this may not be covered, and what the out-of-pocket costs to correct this may be
A discussion of the lengthy list of possible side effects, both the physical side-effects and psychosocial impacts including addiction and increased suicidality (and I would insist that when deciding what side effects merit mention, the same data threshold that is used for recommending the surgeries be applied. This avoids a situation where harms aren’t mentioned because the evidence for them is considered “insufficient,” utilizing a much more rigorous test than is applied to the evidence for recommending the procedures.)
Truly addressing patients’ desperation to experience less weight stigma (including when it is due to the healthcare system’s messaging that fat patients should be willing to risk their lives and quality of life to be thin, and/or holding other healthcare hostage until weight is lost) and offering alternatives including weight-neutral interventions, advocacy for the procedures they actually want/need, and size acceptance/ fat liberation community resources
If “testimonials” and/or “success stories” from surgical patients are given, testimonials and/or stories should also be provided from those who have horrific lifelong side effects and regret the procedure, as well as from the family of friends of those who have passed away. Preferably, testimonials and/or stories from patients utilizing weight-neutral interventions would also be included. (Again, remembering that the goal here is informed consent, not selling the patient on the surgery.)
If the patient is having the surgery to treat/prevent health issues, it should be made very clear that there are thin patients who have the same health issues that this patient does, and that they are not asked to risk these surgeries, and giving the higher-weight patient the option to continue medical management in the same manner as those thin(ner) patients
Making sure the patient has access to options for weight-neutral healthcare. I wrote this article with endocrinologist Dr. Gregory Dodell to talk specifically about weight-neutral glycemic management. For many other conditions you can check out the HAES Health Sheets which I co-created with Dr. Louise Metz and Tiana Dodson.
This three-part series has been an introduction to the subject of these surgeries. Unfortunately, as long as the healthcare system continues to believe that it’s worth risking fat patient’s live and quality of life with these dangerous procedures, there will continue to be more to say. If there’s something specific you would like me to write about, please feel free to leave it in the comment section.
Did you find this post helpful? You can subscribe for free to get future posts delivered direct to your inbox, or choose a paid subscription to support the newsletter (and the work that goes into it!) and get special benefits. Click the Subscribe button below for details:
More research and resources:
https://haeshealthsheets.com/resources/
*Note on language: I use “fat” as a neutral descriptor as used by the fat activist community, I use “ob*se” and “overw*ight” to acknowledge that these are terms that were created to medicalize and pathologize fat bodies, with roots in racism and specifically anti-Blackness. Please read Sabrina Strings’ Fearing the Black Body – the Racial Origins of Fat Phobia and Da’Shaun Harrison’s Belly of the Beast: The Politics of Anti-Fatness as Anti-Blackness for more on this.
Part 3 is the first one of this series I have read but I am looking forward to going back to read 1 and 2. I practice as a weight-neutral dietitian using IE and HAES principles a foundation in my work. I have had clients come to me wanting to get weight loss surgery and I often find it difficult to convert them to an anti-surgery approach. They want to believe that my way is the right way but they are filled with empty promises by the people that are promoting weight loss surgery. This article is perfect and I'd love to share but I think non-believers would loose interest quickly and stop reading. Would you consider creating something shorter, maybe a 1-pager, with key points that could be shared with clients considering bariatric surgery? Thank you for sharing!!!
Hello. I'd appreciate your insight into some claims about BS. Trigger warning for talk about IWL and potential anti-fatness.
.
.
.
.
I'm confused because of the conflicting info I've read and feel pressure myself to pursue IWL as a super fat person, even if that means getting surgery, though I've no plans to do it -- still not convinced it's a good idea overall.
The first claim is that about 50% of people regain the weight, which means around 50% are able to keep it off.
What I've read from other people who have had it (or known those who have had it) is that, in order to have success, one must change their mental and emotional framework and get to the root cause of their bad relationship with food. Tammy Slaton is being touted as proof of success when mindset is changed.
A woman whose comment I read said that she and/or some of her friends (sorry -- can't remember) all got bariatric surgery and the only friend who gained the weight back was the one who "didn't take care of herself."
The implication is that, if you do what you're supposed to, you will maintain the loss.
What do you think? I've read about multiple supposed success stories from the surgery, with quite a few 10+ years out and maintaining the loss (or most of it). I ask myself if someone can hang on for a decade -- longer, even -- and still eventually experience regain.